 Our dietary habits are one of the most important influences relative to our health. Most of the diseases associated with aging have their roots in our food choices. The leading causes of mortality in our country are heart attacks, cancer and strokes, and all have been shown to be modifiable with diet. We often hear warnings about reducing the amounts of certain things in our diets, such as cholesterol, saturated fats and sugars. While the moderation of these is essential to a healthy body, it is also important to increase our intake of foods that have advantageous properties in order to reap their nutritional benefits.
Studies that look at the health of populations routinely reveal that people with diets based on fruits, vegetables, whole grains, nuts, seeds, beans and fish live longer and have significantly less cancer, heart disease and strokes. For example, Okinawa, Japan, where the aforementioned foods represent the average diet, has the largest population of centenarians in the world. The old adage "we are what we eat" is absolutely true. According to a study published in the European Journal of Cancer Prevention, "A large body of evidence indicates that a high intake of fruits and vegetables is associated with a reduced risk of cancer at several sites ." A higher intake of fruits and vegetables directly correlates to a lower risk of cancers, especially of the digestive and respiratory tracks. While it is important to reduce the consumption of certain foods, a diet rich in antioxidants, fiber and omega-3 fatty acids is essential to good health. Antioxidants Abundant in many fruits and vegetables, antioxidants are a vital component to a healthy diet because they stabilize free radicals. Free radicals are unstable electrons formed during the process of oxidation (a natural process associated with aging and metabolizing foods), as well as from drinking alcohol, exposure to pollution and radiation, smoking, iron overload and extreme exercise. During oxidation, a free radical takes an electron from another source in order to become stable. This process can, in turn, form new free radicals, cause DNA to become unstable and turn a cell cancerous or cause oxidation of the bad form of cholesterol, which makes it stickier and creates cholesterol plaques in the arteries. This oxidation process leads to Alzheimer's disease, cardiovascular disease, cancer, cataracts, arthritis, macular degeneration and immune dysfunction, just to name a few. Antioxidants can donate an electron to free radicals while still maintaining their own stability. The free radicals are then stabilized, hopefully before much damage has been done. Antioxidants are plentiful in colorful fruits and vegetables, the more colorful, the better. The antioxidant chemicals are usually found in the pigment, and are much more plentiful in organic produce. Interestingly, antioxidants are produced by the plant as a natural insecticide. If the plant is exposed to chemical insecticides, it gradually loses the need to produce antioxidants for survival. There are many different kinds of antioxidants, and each offer particular benefits. Lycopene, a powerful antioxidant, is a pigment that gives some fruits and vegetables their red color. It is found in tomatoes (and found in higher concentrations in cooked tomatoes), pink and red grapefruit, guava and watermelon. The lycopene content of tomato products may account for the benefits seen in 57 out of 72 studies recently reviewed by Giovannucci at Harvard Medical School. "The evidence for a benefit was strongest for cancers of the prostate, lung and stomach…and suggestive of a benefit for cancers of the pancreas, colon, rectum, esophagus, oral cavity, breast and cervix." With our top cancer killers being in the lung, colon and breast, diets high in tomatoes seem more than prudent. Polyphenols, another class of antioxidants, have also been associated with a lower risk of some diseases, including cancer. These compounds, which are in high concentration in green tea, are also found in fruits and vegetables. Tea polyphenols have been shown to lower LDL (bad) cholesterol and lower the risk of specific types of cancer. They detoxify the metabolites of cancer, decrease cell replication and therefore cancer growth, and improve the ratio of good versus bad bacteria in the gut. Phytoestrogens, a category of compounds that fall within the polyphenol class, is also showing promise in the fight against cancer. Studies have shown that eating a diet high in these plant estrogens (e.g. soy, hops and black cohosh) may decrease the risk of developing breast cancer and prostate cancer. However, the benefits of these plants remain controversial for a person who has been diagnosed with an estrogen receptor positive breast cancer. Fiber Diets high in fiber are helpful in bowel regulation and seem to be protective against colon cancer. Populations that have a very low intake of fiber have high rates of colon cancer and vice-versa. A diet high in red meat and processed meats increases your risk of getting colon cancer, while a diet rich in fiber lessens your risk of the disease. Fiber supplements do not confer the same level of protection against cancer. In almost all studies performed to date, getting nutrients from food supplements in general does not provide the same benefit as obtaining them from the food or plant (as in tea). This is likely because the compounds in the whole food work together in ways that cannot be replicated by a supplement taken out of context. Fats Fats are metabolized into products that can be categorized as either pro-inflammatory or anti-inflammatory. Animal fats and trans fats (such as partially hydrogenated vegetable oils) produce pro-inflammatory cytokines, which can lead to chronic illnesses. These fats are found in red meat, poultry, dairy products, margarines and almost all packaged foods. Interestingly, free-range meat (animals eating grass and allowed to exercise) has a higher percentage of omega-3 fatty acids and lower saturated fat than meat subjected to standard animal husbandry techniques (animals fed grains and remains of other animals, and also not allowed to move). Omega-3 fatty acids are in the category of essential fatty acids, meaning that we must get these from foods because our bodies cannot produce them. Omega-6 fatty acids, found in many vegetable oils, are also considered essential, but we currently have an overabundance in our standard western diet. The ratio of omega-6 to omega-3 is important. In an ideal situation, the ratio is 3:1, but in our diets it is closer to 20:1. Fish, flaxseed and walnuts are excellent sources of omega-3 fatty acids, which have been shown to help reduce heart attacks, arrhythmias (irregular heart beats), strokes, Alzheimer's disease, and reduce inflammation in a whole host of autoimmune disorders such as rheumatoid arthritis, lupus and sarcoidosis. Maitake mushrooms have significant immunostimulant properties by activating natural killer cells, cytotoxic T-cells, interleukin-1, superoxide anions and macrophages. In animal studies, they show marked inhibitory activity against sarcomas. In combination with chemotherapy, they can increase the effectiveness of lower doses of Western drugs, while protecting the immune system from toxic damage . However, further studies are needed to identify the unique contributory effects and mechanisms of action of fractions and other maitake constituents. Watch What you Eat A healthy diet also requires monitoring and elimination (or at least a reduction) of foods that can be harmful. Recent reports regarding polychlorinated biphenyl (PCB) contamination in 70% of the farm-raised fish studied are also concerning. These should be avoided. Mercury is also a concern for many lake and ocean fish, while herring, sardines and canned chunk light tuna are very low in mercury. Alaskan salmon (fresh or canned) is also safe, but tuna steaks, halibut and mackerel have been shown to have elevated mercury levels. Studies using fish oil supplementation show a benefit when at least 2,000 mg are used. These do not appear to be a significant source of mercury or PCBs. In order to create and maintain good health, it is important to eat a healthy, well-balanced diet that includes a variety of fruits and vegetables. Sometimes, Moms really do know best! Christiaan Janssens CRO Akwa Wellness Sources and References LaVecchia C, Tavani A, Fruit and vegetables and human cancer. Eur J Cancer Prev. 1998 Feb;7(1):3-8. Asami DK et al: J Agric Food Chem, 51:1237-1241, 2003. Giovannucci E, Tomatoes, tomato-based products, lycopene, and cancer: a review of the epidemiologic literature. J Natl Cancer Inst. 1999 Feb 17;91(4):317-31. Ahmad N, Mukhtar H, Green tea polyphenols and cancer: biologic mechanisms. Nutr Rev. 1999 Mar;57(3):78-83. Weisburger JH, Tea and health: the underlying mechanisms. Proc Soc Exp Biol Med. 1999 Apr;220(4):271-5. Grant KL, McDermott JH, Alternative Medicine in Nutrition Support. Pharmacotherapy Self Assessment Program (PSAP) 3rd ed. 1999. 7 Weil A, Spontaneous Healing, 1995, Alfred A. Knopf, Inc. Grant KL, McDermott JH, Alternative Medicine in Nutrition Support. 1999. Ahmad N, Mukhtar H Nutr Rev. 1999 Mar. Monograph: Fish Oil; Alternative Medicine Review. 2000 Dec. 5:576-80. Grant KL, McDermott JH, Alternative Medicine in Nutrition Support. 1999. Weil A, Spontaneous Healing, 1995, Alfred A. Knopf, Inc.
1 Comment
Introduction Eating is undoubtedly one of life's greatest pleasures. The sight, smell, taste, and texture of food are just a few characteristics that entice us eat what we eat. History, religion, culture, friends, family and the environment also influence our food choices. And hopefully, we also base our food choices on nutrition and health. A healthy diet provides the right balance of carbohydrates, fats, protein, vitamins and minerals. This balance can be obtained from eating a variety of foods that are available, affordable, and enjoyable. Knowing how to select and plan a healthy meal can be important for staying healthy and/or improving your health. 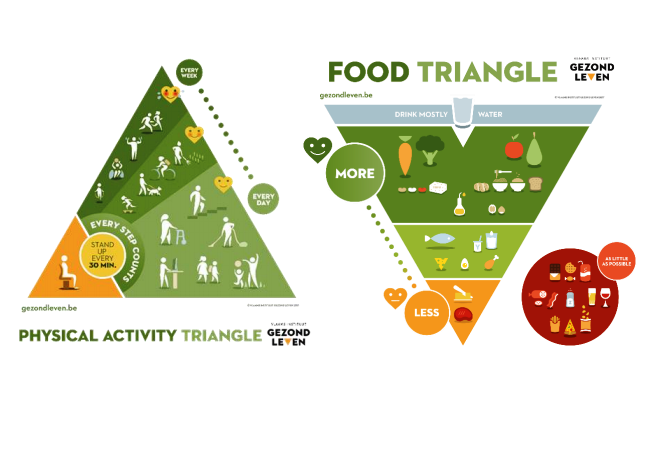 Source: Flemish Institute Healthy Living Source: Flemish Institute Healthy Living How to maintain a healthy diet To maintain a healthy diet, consider the following: Variety: Eat a variety of foods from all groups of The Food Triangle. No single food contains all of the nutrients your body needs to function properly. Eating foods from the five food groups ensures that your body is getting all the nutrients it needs. It also provides a large variety of tastes and textures to enjoy! Balance: All adults need to consume at least the minimum number of servings from each food group every day. The goal is to obtain adequate amounts of nutrients by making food choices from each food group in The Food Triangle. Children, adolescents and seniors have different nutrient requirements. Triangles are available for these specific populations as well: for children or adolescents click here. Moderation: Remember, there are no good foods or bad foods. Watching portion sizes of some of your favorite "not so healthy" foods or beverages will help you to maintain the appropriate weight for your age, gender, and activity level. Safety: Be sure to keep foods safe to eat through proper handling, storage and cooking methods. Also, use proper handwashing techniques and sanitation. To maintain good health, use the Food Triangle to guide your food choices. Nutrients and Other Food Components All foods contain nutrients and other components. Nutrients can be broken down into two groups- macronutrients and micronutrients. Macronutrients include carbohydrates (starches and sugars), proteins (meat, dry beans, eggs), and fats (oils and margarine). Macronutrients provide energy (calories). Micronutrients include vitamins and minerals. These are needed in much smaller amounts, and unlike macronutrients do not provide energy. It is best to obtain these nutrients from whole foods rather than vitamin or other supplements. Other components found in foods that are not classified as nutrients include water, fiber and phytochemicals. Fiber is the indigestible part of plants that helps maintain bowel health and may reduce the risk of diabetes, heart disease and some cancers. Plant foods also contain several phytochemicals that may aid in the prevention of cancer, heart disease and other chronic conditions. Phytochemicals make up the taste, texture and smell of foods. Ongoing research is being done to determine the roles that these substances play in maintaining health. Like vitamins and minerals, phytochemicals should be obtained from a variety of plant-based foods, rather than supplements. You Are What You Eat Studies show that a healthy lifestyle, which includes balanced meals and regular physical activity, can play a role in reducing the risks of several chronic diseases and premature death. Poor eating habits and lack of physical activity are risk factors for several chronic diseases among adults including: - Obesity - Heart disease - Stroke - Hypertension - Diabetes - Some cancers - Osteoarthritis While the focus of the media is so often on weight loss, people concerned about health should focus on healthier eating habits and physical fitness for a lifetime. You can learn more about adopting a healthier lifestyle by talking to a registered dietitian and your health care provider. Christiaan Janssens
CRO Akwa Wellness Sources and References: Belin, R.J., et al., Diet quality and the risk of cardiovascular disease: the Women’s Health Initiative (WHI). Am J Clin Nutr, 2011. 94(1): p. 49-57. World Cancer Research Fund and American Institute for Cancer Research, Continuous Update Project Report Summary. Food, Nutrition, Physical Activity, and the Prevention of Colorectal Cancer, 2011. "Nutrition Plate Unveiled, Replacing Food Pyramid". The New York Times. 2 June 2011. Websites: The Food Pyramid Healthy Eating Plate & Healthy Eating Pyramid Healthy Living 2017 Healthy Eating Introduction The skin is a fascinating organ, unmatched in its complexity, yet necessary for all aspects of daily life. Much of the time, the skin functions so well that we only notice it when we are uncomfortable. The skin is our interface or boundary between us and the environment and us and other people. We are always looking for new and better products, practices and solutions to the stress which everyday life places on our skin. This topic covers: - How the Skin Functions - Aging and Its Effects on the Skin - How to Care for and Protect Your Skin - Strategies for Achieving Skin Health How the Skin Functions The skin is the largest single organ of the body, critical for survival, and covers an average area of 21 square feet (think of the floor area of a closet that is 4 feet deep by 5 feet wide). It is the largest organ of immunity from disease and protects by: - Keeping water and essential nutrients inside and unwanted, toxic substances outside - Regulating the temperature for warming and cooling - Repairing damage from cuts, burns, environmental insults, or other trauma  The skin differs from organs like the heart or lungs because it constantly mends itself by replacing the outer layer daily. It is continually ready to respond to harm. Cuts close over, producing new, pink skin. Sunburned skin becomes dry and peels, giving way to a pink, soft, smooth, and supple replacement layer. The environmental insults signal through the surface to layers below which, in turn, begin the restoration process. The skin's outer layer is a "biological space suit" for life on earth, much like space suits protecting astronauts from the hazardous conditions in outer space. These environmental insults include: - Sun exposure - Climatic changes: heat, cold, high or low humidity (moisture level in the air) - Physical abuse: frictional forces in chafing, rubbing, weight bearing, and shaving hair from the skin - Products like soaps, dish washing detergents, household cleaning products, paint, grease, solvents, rubbing alcohol, and cosmetics - Skin-tight clothing - Water in some situations: extended exposure to water has been shown to damage the skin - Lifestyle or habits: smoking, drinking alcohol, lack of sleep These insults, including sun exposure, can suppress the immune system which can result in skin cancer. Protection of the skin from these insults is, therefore, critical for good health. 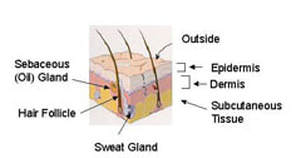 Skin Structure An understanding of the skin structure and function is essential for the health care consumer to provide the proper care for his/her skin. The skin has three major layers: - Epidermis - Dermis - Subcutaneous tissue Each layer has unique functions. This diagram shows a cross section: The epidermis is the outermost layer and it directly interacts with the environment. The epidermis protects by providing a barrier to outside materials (products, water, etc.) and by filtering sunlight. The epidermis is self-renewing. It replaces itself continually, unlike any other organ of the body. The dermis is beneath the epidermis. It contains the major structure-providing tissue fibers, collagen and elastic. It also contains the vascular system to provide a blood supply and nerve cells to process information to and from the brain. The subcutaneous tissue contains the fat pad and muscle. 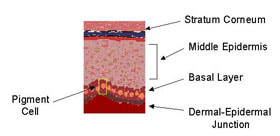 The Epidermis Like all tissues, the epidermis is made up of cells which have specific functions in the skin. A cell called the keratinocyte makes up most of the epidermis. The functions of the stratum corneum, the middle epidermis, the basal layer, and the dermal-epidermal junction are highlighted. The Stratum Corneum The stratum corneum is the outermost layer, directly in contact with the environment. It is about half the thickness of a piece of notebook paper. On average, the stratum corneum is about 20 cell layers thick. Despite its thin dimensions, the stratum corneum is incredibly strong. The cells are in a very well organized pattern. 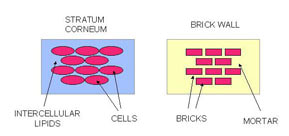 The stratum corneum is the outermost layer, directly in contact with the environment. It is about half the thickness of a piece of notebook paper. On average, the stratum corneum is about 20 cell layers thick. Despite its thin dimensions, the stratum corneum is incredibly strong. The cells are in a very well organized pattern. The stratum corneum has been described as a "brick and mortar" structure, as shown here: The cells are the bricks and the lipids are the mortar. Lipids are "oily" materials that do not easily mix with water, such as cooking oil, petroleum jelly, baby oil, and grease. The skin lipids are mixtures of materials that form a very well organized structure between the cells. The lipid layer helps keep water in the stratum corneum by limiting passage of water from beneath. The lipids also keep water and water loving substances out of the body. The stratum corneum contains water that is associated with the protein materials in the cells. The cells hold onto water to keep them flexible and to allow the body's movement without cracking the upper layer. 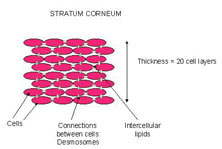 Neighboring stratum corneum cells are joined together through small attachments, called desmosomes. In a sense, these are like small "rivets". Each cell is attached at many points to nearby cells (cells above, beneath, adjacent). These multiple attachments provide considerable strength to this tissue. The very top layer of the stratum corneum normally comes off or "sheds", about one cell layer per day. You can observe this layer by placing a piece of clear tape and put it on the back of your hand for a few minutes. Remove the tape and notice the flaky material, which is the top layer of cells. The desmosomes need to break in order to free the cells. This process, called desquamation, is carefully programmed to occur at the proper time. The Middle Epidermis Right below the bottom of the stratum corneum lies the middle epidermis. At the top, the cells are flatter than the rest of the layer. These top cells contain lipids and release them as they move upward. These lipids then become the stratum corneum lipids. The remaining cells are keratinocytes which have a cube shape and contain bundles of filaments that help protect the skin from the friction during movement and rubbing. Over time, the cells move upward to the top of the middle epidermis and eventually become stratum corneum cells. Their features change over time during this renewal and replacement process. The Basal Layer The basal layer rests at the bottom of the middle epidermis. The basal cells are different, however, because they actively divide to create new basal cells. The older cells move up to form the middle epidermis. All cells of the epidermis begin at this point by the process of cell division. The cell division process needs protein and other nourishment that are supplied by the functions of the dermis. The basal layer contains a unique type of cell called the melanocyte or pigment cell. Unlike other basal cells, the melanocyte does not move upward. The melanocyte's job is to make a substance called pigment, or melanin, which contributes to the coloration of the skin. Melanocytes go into action to make melanin when ultraviolet radiation interacts with the skin. The melanin is transferred from the melanocyte to the keratinocytes of the middle epidermis, to protect the nuclei of these cells from being damaged by radiation. Dark spots on the skin, such as freckles, are clusters of epidermal keratinocytes with melanin concentrated in them. Sun tanned skin has a more uniform distribution of keratinocytes with melanin. Both conditions are the response of the skin to sun exposure. As the name suggests, the dermal-epidermal junction is right between the epidermis and the dermis. This layer of the skin holds the epidermis onto the dermis. It provides support to the entire tissue to help hold it in place. Epidermal Cell Summary The epidermis performs a wide variety of functions. Epidermal cells, or keratinocytes, move from the basal cell layer to the top of the stratum corneum in about 28 days. The specific time depends on the location on the body, the overall state of health, and the type and severity of environmental insult. The outermost layer of the stratum corneum comes off each day. When injury to the skin occurs, again from some sort of damage, the whole replenishment process works overtime to restore the skin to its proper condition and to ensure a protective barrier. In the case of serious injury, such as a major burn, the healing process requires a long time. The melanocytes, or pigment cells, housed in the bottom of the epidermis, produce melanin to protect the epidermal cells from ultraviolet damage. The epidermis is unusual in that it does not contain nerve endings. Yet, the outer surface of our skin, the stratum corneum, can very easily detect events, including changes in heat, cold and humidity. We can also tell when the skin is touched. Even though it does not have nerve endings, the epidermis is thought to play an important role in signaling between the outside  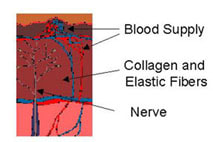 The Dermis The dermis is below the epidermis and above the subcutaneous tissue. The epidermis is unusual in that it does not contain nerve endings. Yet, the outer surface of our skin, the stratum corneum, can very easily detect events, including changes in heat, cold and humidity. We can also tell when the skin is touched. Even though it does not have nerve endings, the epidermis is thought to play an important role in signaling between the outside world and the brain. Collagen and elastin fibers make up a large part of the dermis. The thick fibers of collagen support the skin. Elastin fibers are very flexible and impart mechanical strength and resiliency to the skin by allowing it to stretch. When the elastin is in good condition, the skin returns to its original shape readily when it is flexed or stretched. If the elastin and collagen are in poor condition, the skin lacks resiliency, sags, and develops noticeable wrinkles. The major functions of the dermis are to support the epidermis, to provide bulk and to anchor the skin. Importantly, the dermis contains blood vessels that bring oxygen and other nutrients to the basal layer for the cell division process. Nerve endings are also found in the dermis. Presumably they take signals from the epidermis, including the stratum corneum, and transmit them to the brain. This signaling function is unique because there are no nerve cells in the epidermis. The major parts are shown here: 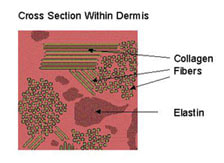 The diagram shows that the dermis has a compact array of fibrous material, the collagen and elastin, necessary for support, resistance to damage, and overall health. Aging and Its Effects on the Skin The effects of aging on the skin are currently of great interest. People are living longer and more active lives than ever before. The "baby boomers" are now in their 30s, 40s and 50s. They have large disposable incomes and no intention of looking old. For them, "looking good" and "feeling good" go hand in hand. The process of skin aging process has two parts: natural aging, due to increasing chronological age, and solar aging, due to the effects of the sun. Natural Aging Natural aging includes all of the environmental and genetic factors that impact the skin, other than those due to solar damage. As the skin ages, the cell movement from the bottom of the epidermis (basal layer) to the top (outermost stratum corneum) becomes slower. The skin surface becomes rougher, with a more uneven texture, because the cells are shed more slowly. Often the slowed desquamation process (remember the tape on your hand experiment?) results in the formation of large clumps of cells, observed as scales or dry skin flakes. The uneven texture and scaling tend to make your skin look duller. The epidermis becomes thinner and the skin becomes more fragile. In the dermis, the elastic fibers become coarse and then disappear. The coarseness makes them less elastic. The skin returns to its original state much more slowly when it is stretched. The blood vessels decrease in size and number. This change influences the nutrient supply to the basal layer and accounts in part for the slower rate of epidermal replenishment. Some of the factors in natural aging are determined by the genetic make up of the individual. Much more needs to be learned about specific genetic influences. Photoaging & Sun Damage Sunlight causes significant damage to the skin which, unfortunately, does not show up right away. In fact, many people believe sun or tanning bed exposure equals a healthy appearance and healthy skin. This "socially desirable appearance" comes at the expense of poor appearance and poor skin health as one gets older. Tanning beds provide ultraviolet radiation through special bulbs and damage the skin as much as the sun itself. Individuals who spend most of their time indoors are still exposed to damaging rays when they do go outside. Sun damage takes two forms, photoaging and skin cancer. The majority of a lifetime sun exposure occurs before the age of 20. Children receive three times more exposure to the sun than adults. The damage process starts early in life unless the skin is protected. Many non-melanoma skin cancers could be prevented with proper protection from the sun. Photoaging: The Epidermis Ultraviolet radiation from the sun penetrates the stratum corneum. It affects the epidermal cells and causes a change in thickness. Some areas of the epidermis increase in size and others decrease to produce an irregular, non-uniform structure. The normal, orderly processes of the epidermis are disrupted. As a result, the epidermis cannot produce a proper stratum corneum. The "defective" stratum corneum is irregular and the very top layer does not slough off properly. Consequently, the skin surface texture becomes rough and irregular. The skin pigmentation, or coloration, becomes blotchy and irregular. This happens because the melanocytes are forced, by the ultraviolet radiation of the sun, to produce pigmentation. The pigment is transferred to the keratinocytes of the middle epidermis and these spots become visible when we view the skin surface. In addition, the skin tone becomes sallow and appears to lack the vitality of a healthy state. Photoaging: The Dermis Sunlight breaks down the collagen and elastin fibers in the dermis. These structures become irregular. This irregularity in the dermal support tissue leads to visible wrinkles. The fibers also lose their elasticity, causing the skin to sag. Sun damage leads to chronic inflammation of the dermis. As a consequence, the epidermis does not function properly. The chronic inflammation causes the epidermis to become thicker as it attempts to repair the damage. Levels of Photoaging Photoaging occurs to varying levels. 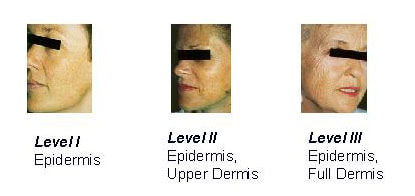 In Level I, ultraviolet radiation causes changes in the epidermis only. The alterations result in a dull, rough outer layer and in pigmented spots. In Level II, changes are caused in both the epidermis and the upper part of the dermis. Injury from the sun leads to increased wrinkling, and alterations in pigmentation and texture that are greater than those in Level I. Consequently, the skin's features are not uniform, thereby exaggerating the effects. In Level III, changes occur in the epidermis and throughout the dermis. The wrinkling is more pronounced and the skin texture is much less uniform, often pebbly in appearance. The skin takes on a leathery appearance. How to Care for and Protect Your Skin Skin care begins with a healthy lifestyle. Strive to do the following, wherever possible: drink plenty of water, eat a balanced diet with sufficient vitamins, exercise regularly, get enough sleep, avoid smoking and the use of tanning beds, minimize alcohol consumption, and manage daily stress. Some of these lifestyle techniques are easier to sustain than others, but they represent useful goals. Care for your skin in each of the following areas.  Skin Cleansing For daily hygiene, use a mild cleanser. Remove facial make up completely. Use lukewarm water for all cleansing. Rinse the skin thoroughly to remove cleansing materials from the skin surface. Gently pat dry and avoid rubbing. Skin Moisturizing In "moisturizing," water is added to the skin. Moisturized skin is more flexible than dry skin. Application of moisturizer immediately after washing helps keep water within the skin. Skin moisturizers: 1 improve hydration (moisture content) 2 add a "protective" layer on the skin surface to help hold moisture within the top layers. A large number of emollient creams and lotions are available. The protective layer provides a barrier to water loss. Therefore, water remains in the upper layers of the epidermis and makes the stratum corneum more flexible. Read product labels to check for certain ingredients. One of the most common ingredients for increasing hydration is glycerin, which holds onto water within the outer layers following application. A second type of ingredient serves as a barrier when applied to the skin. These materials include petrolatum, mineral oil, and certain plant oils. They are lipid in nature and protect the skin by minimizing water loss from the epidermis and by providing a barrier to intrusion.  A second group of skin care materials is alpha hydroxy acids, known as the fruit acids (glycolic acid, lactic acid, etc.), and beta hydroxy acids (salicylic acid). These materials create a smoother skin surface by hydrating the surface layers and weakening and breaking the attachments between the stratum corneum cells. This process, known as exfoliation, assists in the removal of surface dry, scaly patches.  Cancer Awareness We advise periodic evaluations of any marks, moles, or pigmented areas by a trained health care professional. Any mole that changes in size or has an irregular border must be checked. Prevention of skin cancer involves avoiding sun damage and detecting trouble spots early. Be aware of changes in your skin and have them evaluated. Adult Skin Care An individual's skin care regimen should include basic elements, as well as those tailored to specific needs and lifestyles. For the early adult (20-35 years), we recommend cleansing with a non-soap product and rinsing well and moisturizing, particularly in cold weather. Application of sun screens and sun blocks on a daily basis at an SPF value of 15 is essential. For early signs of damage, such as uneven pigmentation or fine wrinkles, a retinoid product should be considered. Control of acne is often an important element. For the middle adult years (35-65), cleansing, moisturizing, sun protection, and use of retinoids are recommended. Acne can be problematic for this group, as well as early adults and teenagers. For persistent acne, various medications and treatments are available. Individuals may consider restorative techniques, such as the chemical peel, dermabrasion, or laser resurfacing, to correct the damage caused by sun exposure. For the older adult (over 65 years), the cleansing, moisturizing, and sun protection routines should be followed. Restorative techniques can provide noticeable improvement in skin damaged by sun exposure. Regardless of age, sun exposure should be minimized and sun screens and sun blocks applied routinely. They will prevent additional damage. Infant Skin Care At birth, the full-term human newborn is well-suited for life in a dry environment. The infant's skin provides an efficient and protective barrier during the transition from the water environment to life outside. The full-term infant's skin functions very well. The stratum corneum barrier protects against water loss and infection. The effective functioning of this barrier is surprising, particularly because the infant has spent nine months in a very wet environment. Nature has provided mechanisms to protect the infant's skin in utero and to allow the stratum corneum to develop properly. For infants born prematurely, the skin barrier is immature. The more premature the infant is, the poorer the skin barrier. Poor barrier function results in high evaporative water loss, which has negative consequences for temperature control and metabolism. Infants born less than 30 weeks gestation have a significantly poorer stratum corneum barrier than those born at term and at 32-34 weeks gestation. Once the baby is born and exposed to dry conditions, the barrier forms rapidly. This maturation takes place within the first five days of life for the preterm infant of less than 27 weeks. Bathing For routine bathing of the infant's skin, we suggest a liquid product. Several brands are commercially available. The product should be diluted with water before it is applied. The infant should be rinsed thoroughly with water to minimize any cleanser residue left on the skin that may disrupt barrier function. Diaper Area Care Diaper rash is a common occurrence among infants and young children. Most of the time, the rash is relatively minor and appears as reddened areas within the diaper region. For mild irritation, we suggest cleansing the skin with warm water and a soft cloth. The skin should be dried thoroughly before diapering the baby. A hair drier on a very low setting is effective for drying the skin. At other times, particularly if the infant has been taking antibiotics and experiences diarrhea, the rash can be more severe. The area should be cleansed with warm water and a soft cloth. Apply a diaper rash product to the affected areas. This will provide a "protective" barrier between the skin and the next soiling. Use a product that is easy to cleanse away and do not rub the skin. Ideally, only remove the soiled material. Leave the remaining cream in place to avoid scrubbing the skin. Reapply the rash cream as needed. If the rash does not clear up or if it gets worse, seek medical attention. Sources and References:
Marks, James G; Miller, Jeffery (2006). Lookingbill and Marks' Principles of Dermatology. (4th ed.). Proksch, E; Brandner, JM; Jensen, JM (2008). "The skin: an indispensable barrier". Experimental Dermatology. 17 (12): 1063–72. Maton, Anthea; Jean Hopkins; Charles William McLaughlin; Susan Johnson; Maryanna Quon Warner; David LaHart; Jill D. Wright (1893). Human Biology and Health. Englewood Cliffs, New Jersey, USA: Prentice Hall. Jablonski, N.G. (2006). Skin: a Natural History. Berkeley: University of California Press. Shapiro SS, Saliou C (2001). "Role of vitamins in skin care". Nutrition. 17 (10): 839–844. McGrath, J.A.; Eady, R.A.; Pope, F.M. (2004). Rook's Textbook of Dermatology (7th ed.). Martin, P. Wound Healing-aiming for perfect skin regeneration. Science (1997), 276, 75-81. Websites: The Aging Skin The Human Skin Skin Information and Facts  Asthma is an inflammatory condition of the lungs, characterized by narrowing of the airway passages. This disease is at least partially reversible if treated with appropriate medications.
Symptoms Asthma, which is estimated to afflict over 9 million Americans, has many patterns of presentation and can occur at any age. Commonly experienced symptoms of asthma include:
Since other diseases can cause similar symptoms, it is always important to be examined by a physician. Causes Asthma may be caused or triggered by allergic and non-allergic factors. Allergic factors or challenges include:
Upon repeated exposure to these substances, the body forms allergic antibodies called IgE, directed toward specific allergens. An important part of evaluating allergic asthma includes skin testing to allergens to determine if any allergic antibodies are responsible for aggravating symptoms of asthma. Skin tests are always interpreted in light of the patient's history, since falsely positive tests occasionally occur. Non-allergic factors that can trigger asthma include:
There are some patients who develop allergic asthma after exposure to certain proteins and chemicals in their work environment. Some workers develop asthma in the workplace after exposure to irritating fumes. Treatment Two principles guide asthma treatment:
When possible, factors which cause asthma to flare up should be identified and avoided if at all possible. It is very important that patients with asthma learn to recognize the early warning signs and symptoms of asthma attacks, and take appropriate actions before the disease gets worse. Patients whose symptoms are frequent (more than twice a month) and/or who have evidence of airway obstruction should take anti-inflammatory asthma medications on a regular basis. When a treatment program is recommended, it is very important that the physician's instructions be followed in order to get the most relief and best control of asthma symptoms. If asthma should worsen in the future for whatever reason, it is very important to call a physician immediately for advice regarding required changes in your treatment. When these flares of asthma are treated early, severe asthma attacks, emergency room visits, and hospitalizations can usually be avoided. If managed and treated properly, the vast majority of individuals with asthma can lead normal, active, and productive lives. Christiaan Janssens CRO Akwa Wellness Sources and References: Holgate ST. The epidemic of allergy and asthma. Nature 1999; 402 (6760 suppl): B2-4. Strachan DP. Hay fever, hygiene, and household size. BMJ 1989; 299: 1259-60. Martinez FD, Holt PG. Role of microbial burden in aetiology of allergy and asthma. Lancet 1999; 354 (suppl 2): 12-15. Moore, W.C., Meyers, D.A., Wenzel, S.E., Teague, W.G., Li, H., Li, X. et al. Identification of asthma phenotypes using cluster analysis in the Severe Asthma Research Program. Am J Respir Crit Care Med. 2010; 181: 315–323. Ober, C. and Hoffjan, S. Asthma genetics 2006: the long and winding road to gene discovery. Genes Immun. 2006; 7: 95–100. Websites: Guidelines for Diagnosis Management of Asthma Asthma: Causes, Symptoms & Treatment Asthma - Symptoms and causes  A trip to the dentist can sometimes give you more than you bargained for: In some cases, it's a dentist who may be the first to discover that a nagging sore or odd-looking white patch is not merely an annoyance, but an early form of oral cancer.
Dentists are the very best when it comes to finding early lesions in the mouth that could eventually wind up being cancerous. Studies show that dental hygienists and dentists are the most thoroughly trained and the most sensitive to early, subtle changes in the mouth that could signal trouble later on. In other words, they may be able to spot problems that other primary care providers may miss. And when it comes to oral cancer, the earlier it's discovered and treated, the better the chances of making a full recovery. Oral cancers make up only a small fraction of the number of new cancers every year, but they are some of the deadliest. Currently, about half of all oral cancers are first detected after they have already had opportunity to take root and spread. At that point, they are difficult to cure. The American Cancer Society estimates that only about half the people diagnosed with oral cancer will survive longer than five years. New treatments are desperately needed. A variety of agents that range from anti-angiogenesis drugs such as endostatin, to natural products like extracts from freeze dried black raspberries are being investigated to see if they may be able to suppress the conversion of precancerous to cancerous cells. Recently a clinical trial was approved to see if the black raspberry extracts can block the progression of precancerous oral lesions in humans. Since the risk of oral cancer increases with age, clinicians are expecting an increasing number of cases in the coming years because large numbers of baby boomers are just beginning to enter their most vulnerable, cancer-prone decades. This is a time when increased attention to periodic screening is so important. While oral cancer is still more prevalent among men, dentists are seeing an increasing incidence among women, probably because more women are choosing to smoke. People at higher risk of developing oral tumors include anyone who uses tobacco products in any form and who drinks alcohol on a regular basis. Catching oral cancer in its earliest phase is critical, as shown by the success of screening in reducing deaths from other types of cancer. What has happened with cervical cancer in recent years is a good example. In many, less developed countries, cervical cancer still takes a terrible toll among women. But here in the United States, where there is about a 75-80 percent compliance with regular and routine screening, the incidence of cervical cancer has dropped significantly, and deaths have declined dramatically. About 90 percent of oral malignancies are squamous cell carcinomas, meaning they originate in the lining of the mouth or tongue. And some sites in the mouth - particularly where pooling of saliva may occur - are more vulnerable than others. These areas, including the sides and undersurface of the tongue, the floor of the mouth, the soft palate at the back of the mouth and the tonsils, are the most common cancer sites, representing about half of all cases. Cancer in its earliest stages can make the lining of the mouth or the tongue look just a little bit different - maybe red or white, or with little bumps. Patients need to be on the lookout for any of the following signs or symptoms: - A sore that bleeds easily or does not heal - A change in the color or texture of any part of the mouth or tongue - Pain or numbness in any part of the oral cavity - A white or velvety red patch that does not wear off It is tragic that so many people develop oral cancer when it's so easy to spot during a checkup. One may not be able to catch or cure every single case, but regular screenings would help us be much more effective in controlling this terrible disease. Christiaan Janssens CRO Akwa Wellness Sources and References: Hussain QA, Awan KH. Role of Dental Profession in Oral Cancer Prevention and Diagnosis. J Contemp Dent Pract 2016;17(12):963-964. Chaturvedi P. Oral cancer: premalignant conditions and screening – an update. J Cancer Res Ther 2012;8(6):57-66. Kohn WG. Guidelines for infection control in dental healthcare settings. National Center for Chronic Disease Prevention and Health Promotion 2003 Dec;52(RR17):1-61. Carpenter WM, Silverman S Jr. Oral cancer: the role of the dentist in prevention and early detection. Dent Today. 2001 May;20(5):92-7. Websites: American Dental Association Oral Health Foundation Oral Cancer Foundation Are dental x-rays really necessary? Many diseases, lesions and conditions can only be detected with the use of dental radiographs. It is impossible to see directly between the teeth or under the gums or bone without the use of a dental radiograph. Many times the patient has no signs or symptoms of disease. Without the use of dental radiographs, the dentist is limited to detect only the disease which is visible in the mouth. Dental x-rays can detect disease much sooner than the clinical examination alone. This enables the dental practitioner to identify problems early so that pain and extensive, costly treatment can be avoided. How often should I have dental x-rays? Dental x-rays are prescribed based on the needs of the individual. The dentist must weigh the benefits of disease detection against the risk of radiation exposure. There are guidelines published by the American Dental Association that are used to aid the dentist in prescribing the number, type, and frequency of dental radiographs. However, the dentist knows each patient’s health history and susceptibility to oral disease and is in the best position to make this professional judgment in the interest of each patient. For example, a patient with a high decay rate will need x-rays more frequently than a patient without such disease. How often should children have dental x-rays? There is no set time interval between x-ray exposures. The radiographic exam should be based on the needs of the individual child. For example, children with decay will need x-rays more frequently than children without decay. Can I refuse x-rays and be treated without them? Treatment without the necessary radiographs is considered negligence. If a patient refuses to have necessary dental x-rays taken then the dentist must refuse to provide patient care. Can the dentist use my x-rays from my previous dentist? Yes. If the x-rays are of good diagnostic quality and are recent enough then the dentist may use them for the oral radiographic examination. Some additional radiographs may still be necessary depending on the needs of the individual. How are x-rays measured? Just like there are ways of measuring distance in miles or kilometers and weight in pounds or kilograms, there are ways to measure x-ray exposure. The roentgen is a way of measuring radiation exposure. The amount of energy absorbed by tissue is termed the rad or radiation absorbed dose. How much radiation will I receive from dental x-rays? We are exposed to radiation every day from various sources such as; airplane travel, high altitudes, radon gases and home appliances. 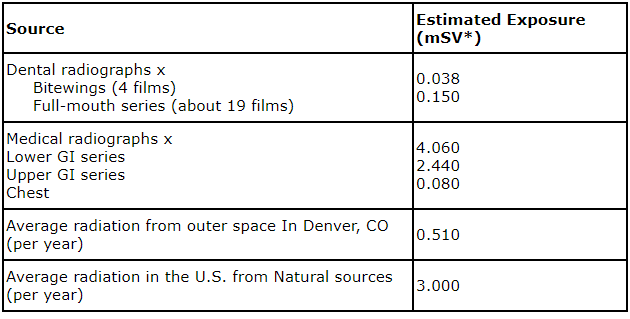 *A millisievert (mSV) is a unit of measure that allows for some comparison between radiation sources that expose the entire body (such as natural background radiation) and those that only expose a portion of the body (such as radiographs).
Why do the dental radiographer use a lead apron? It is important that we do everything that we can to reduce the amount of radiation exposure when a patient has dental x-rays taken. The lead in the lead apron with the lead thyroid collar actually prevents the radiation from reaching the radiosensitive organs, such as, reproductive, blood forming and thyroid tissues from scatter radiation. Should dental x-rays be taken during pregnancy? The accepted cumulative dose of ionizing radiation during pregnancy is 5 rad (.05 Sv). According to the American Academy of Family Physicians, you would need 50,000 dental x-ray examinations to reach the 5-rad cumulative dose to the fetus. The decision to order films during pregnancy is a personal one. Because of the relatively low dose, it is not expected that there will be any harm to the fetus. However, many dentists elect to postpone the radiographic exposures to those needed to treat the patient during the pregnancy (symptomatic teeth or active decay). Why does the dental radiographer leave the room when x-rays are used? Dental x-rays should only be used when the benefit of disease detection far outweighs the risk of any dental x-ray exposure. The dental radiographer will not benefit from the exposure to the x-rays so the best protective measure is to maintain adequate distance and shielding. Can’t my dental office use one large extraoral panoramic radiograph instead of several of the smaller intraoral radiographs? No. A panoramic radiograph cannot be used as a substitute for a complete series of intraoral radiographs. The panoramic radiograph gives an overall view of the teeth and jaws, however it does not show as much detail as the intraoral radiograph. Who owns my dental radiographs? The dental record, including all of the dental radiographs belong to the dentist, however, the patient is entitled to a copy of the dental radiographs. Christiaan Janssens CRO Akwa Wellness Sources and References: Iannucci, JM, Howerton, LJ: Patient Education and the Dental Radiographer. In Dental Radiography Principles and Techniques,Third Edition, St. Louis, 2006, Saunders, pp. 151-153. Frederiksen NL. X-Rays: What is the Risk? Texas Dental Journal. 1995;112(2):68-72.  Most back pain can be treated without surgery.
Treatment involves: Using analgesics
Self-Care Most patients with back pain recover without residual functional loss. Patients should contact a doctor if there is not a noticeable reduction in pain and inflammation after 72 hours of self-care. Ice and Heat: Although ice and heat (the use of cold and hot compresses) have never been scientifically proven to quickly resolve back injury, compresses may help reduce pain and inflammation and allow greater mobility for some individuals. As soon as possible following trauma, patients should apply a cold pack or a cold compress (such as a bag of ice or bag of frozen vegetables wrapped in a towel) to the tender spot several times a day for up to 20 minutes. After 2 to 3 days of cold treatment, they should then apply heat (such as a heating lamp or hot pad) for brief periods to relax muscles and increase blood flow. Warm baths may also help relax muscles. Patients should avoid sleeping on a heating pad, which can cause burns and lead to additional tissue damage. Bed rest: 1–2 days at most. A 1996 Finnish study found that persons who continued their activities without bed rest following onset of back pain appeared to have better back flexibility than those who rested in bed for a week. Other studies suggest that bed rest alone may make back pain worse and can lead to secondary complications such as depression, decreased muscle tone, and blood clots in the legs. Patients should resume activities as soon as possible. At night or during rest, patients should lie on one side, with a pillow between the knees (some doctors suggest resting on the back and putting a pillow beneath the knees). Exercise: Exercise may be the most effective way to speed recovery from low back pain and help strengthen back and abdominal muscles. Maintaining and building muscle strength is particularly important for persons with skeletal irregularities. Doctors and physical therapists can provide a list of gentle exercises that help keep muscles moving and speed the recovery process. A routine of back-healthy activities may include stretching exercises, swimming, walking, and movement therapy to improve coordination and develop proper posture and muscle balance. Yoga is another way to gently stretch muscles and ease pain. Any mild discomfort felt at the start of these exercises should disappear as muscles become stronger. But if pain is more than mild and lasts more than 15 minutes during exercise, patients should stop exercising and contact a doctor. Medications Medications are often used to treat acute and chronic low back pain. Effective pain relief may involve a combination of prescription drugs and over-the-counter remedies. Patients should always check with a doctor before taking drugs for pain relief. Certain medicines, even those sold over the counter, are unsafe during pregnancy, may conflict with other medications, may cause side effects including drowsiness, or may lead to liver damage. Over-the-counter analgesics: including nonsteroidal anti-inflammatory drugs (“NSAIDs”, such as aspirin, naproxen, and ibuprofen), are taken orally to reduce stiffness, swelling, and inflammation and to ease mild to moderate low back pain. Counter-irritants applied topically to the skin as a cream or spray stimulate the nerve endings in the skin to provide feelings of warmth or cold and dull the sense of pain. Topical analgesics can also reduce inflammation and stimulate blood flow. Many of these compounds contain salicylates, the same ingredient found in oral pain medications containing aspirin. Anticonvulsants: drugs primarily used to treat seizures, may be useful in treating certain types of nerve pain and may also be prescribed with analgesics. Some antidepressants: particularly tricyclic antidepressants such as amitriptyline and desipramine, have been shown to relieve pain (independent of their effect on depression) and assist with sleep. Antidepressants alter levels of brain chemicals to elevate mood and dull pain signals. Many of the new antidepressants, such as the selective serotonin reuptake inhibitors, are being studied for their effectiveness in pain relief. Opioids: such as codeine, oxycodone, hydrocodone, and morphine are often prescribed to manage severe acute and chronic back pain but should be used only for a short period of time and under a physician’s supervision. Side effects can include drowsiness, decreased reaction time, impaired judgment, and potential for addiction. Many specialists are convinced that chronic use of these drugs is detrimental to the back pain patient, adding to depression and even increasing pain. Non-Invasive Therapies When back pain does not respond to more conventional approaches, patients may consider the following options: Spinal manipulation: Spinal manipulation is literally a "hands-on" approach in which professionally licensed specialists use leverage and a series of exercises to adjust spinal structures and restore back mobility. Acupuncture: Acupuncture involves the insertion of needles the width of a human hair along precise points throughout the body. Practitioners believe this process triggers the release of naturally occurring painkilling molecules called peptides and keeps the body’s normal flow of energy unblocked. Clinical studies are measuring the effectiveness of acupuncture in comparison to more conventional procedures in the treatment of acute low back pain. Biofeedback: Biofeedback is used to treat many acute pain problems, most notably back pain and headache. Using a special electronic machine, the patient is trained to become aware of, to follow, and to gain control over certain bodily functions, including muscle tension, heart rate, and skin temperature (by controlling local blood flow patterns). The patient can then learn to effect a change in his or her response to pain, for example, by using relaxation techniques. Biofeedback is often used in combination with other treatment methods, generally without side effects. Interventional therapy: Interventional therapy can ease chronic pain by blocking nerve conduction between specific areas of the body and the brain. Approaches range from injections of local anesthetics, steroids, or narcotics into affected soft tissues, joints, or nerve roots to more complex nerve blocks and spinal cord stimulation. When extreme pain is involved, low doses of drugs may be administered by catheter directly onto the spinal cord. Chronic use of steroid injections may lead to increased functional impairment. Traction: Traction involves the use of weights to apply constant or intermittent force to gradually “pull” the skeletal structure into better alignment. Traction is not recommended for treating acute low back symptoms. Transcutaneous electrical nerve stimulation (TENS): TENS is administered by a battery-powered device that sends mild electric pulses along nerve fibers to block pain signals to the brain. Small electrodes placed on the skin at or near the site of pain generate nerve impulses that block incoming pain signals from the peripheral nerves. TENS may also help stimulate the brain’s production of endorphins (chemicals that have pain-relieving properties). Ultrasound: Ultrasound is a noninvasive therapy used to warm the body’s internal tissues, which causes muscles to relax. Sound waves pass through the skin and into the injured muscles and other soft tissues. Infrared Sauna: Using the infrared sauna as your main heat source, you should be able to feel your muscles loosening when they become warmed up. This is made possible with the dilation of blood vessels around the lumbar spine. With the heat penetrating the body and opening up the vessels, the nutrients and oxygen coursing through are able to flow better to the muscles. This begins a healing process for the damaged tissue, as well as eases the transmission of pain signals to the brain. Massage therapy: This therapy can provide substantial healing and pain relief for people suffering from low back pain caused by muscle tension and strain, if the correct muscles are targeted. Christiaan Janssens CRO Akwa Wellness Sources and References: Morrisette D, Cholewicki J, Logan S, Seif G, McGowan S. A randomized clinical trial comparing extensible and inextensible lumbosacral orthoses and standard care alone in the management of low back pain. Spine (Phila Pa 1976). 2014 October 1; 39(21):1733-42. Furlan A, Tazdi F, Tsertsvadze A, et al. Complementary and Alternative Therapies for Back Pain II. Evidence Report/Technology Assessment No. 194. AHRQ Publication No. 10(11) E007. Rockville, MD; Agency for Healthcare Research and Quality. October 2010. Nordin M, Campello M. Physical therapy: exercises and the modalities: when, what, and why? Neurol Clin. 1999;17:75-89. Cherkin DC, Deyo RA, Battié M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med. 1998; 339:1021-9. Bronfort G, Goldsmith CH, Nelson CF, Boline PD, Anderson AV. Trunk exercise combined with spinal manipulative or NSAID therapy for chronic low back pain: a randomized, observer-blinded clinical trial. J Manipulative Physiol Ther. 1996;19:570-82. Websites: www.spine-health.com/conditions/lower-back-pain/non-surgical-treatments-lower-back-pain www.medicalnewstoday.com/articles/172943.php  Back Pain Back Pain The statistics are staggering. About 80-90% experience lower back pain at some point in their lives. Many people with chronic lower back pain are working, and lose productivity on the job as a direct result. In fact, it is estimated by national statistics that back pain costs billions of € a year in lost earnings, and lower back pain is the Number 1 cause of visits to physicians.
Types of Back Pain The most common types of back pain are: -Lumbar pain Lumbar, or lower back pain, is typically located at and above the waist in the middle of the back or spine. The pain can be directly linked to prolonged stretches or sitting, standing, or lifting. -Sciatica Sciatica is a sharp, stabbing pain that starts in the buttock and travels down the leg. It can often include numbness, "pins and needles", and/or even weakness of the leg. Sciatica is one of the most common forms of pain caused by compression of the spinal nerves, and the leg pain often feels much worse than the back pain. Sciatica is actually a symptom and not a diagnosis. While the most common cause of sciatica is a herniated (or "slipped") disc, many other conditions can cause this type of pain. Relieving the Pain If you or a loved one suffers chronic back pain, there are options to relieve the pain in the form of:
Visiting a Spine Specialist Through careful evaluation and diagnostic tests, a spine specialist can determine the correct method of treatment including:
Don't Delay Treatment Regardless of what type of back pain you suffer from, one aspect remains constant: If untreated, chronic aches and back pain can continue to follow you throughout your life. If mundane household chores or tasks at work lead to recurring pain on a daily basis, it's important for you to know that options are available. The vast majority of lower back pain conditions will get better with time and can be addressed with conservative treatments. However, it is important to note that there are some diagnoses that indicate the need for surgery to enable relief from pain and better enjoyment of day-to-day activities. Christiaan Janssens CRO Akwa Wellness April 7th 2018 Sources and References: Burke GL (2008). "Chapter 5: The Differential Diagnosis of a Nuclear Lesion.". Backache: From Occiput to Coccyx. Vancouver, BC: MacDonald Publishing. Lavelle, W. F., Kitab, S. A., Ramakrishnan, R., & Benzel, E. C. (2017). Anatomy of Nerve Root Compression, Nerve Root Tethering, and Spinal Instability. In Benzel's Spine Surgery (4th ed., pp. 200-205). Bogduk, N. (Ed.). (2004). Practice guidelines for spinal diagnostic and treatment procedures. San Francisco: International Spine Intervention Society. Indahl, A., Indahl, A., Velund, L., & Reikerås, O. (1995). Good prognosis for low back pain when left untampered. Spine, 20, 473–477. Chou R, Baisden J, Carragee EJ, Resnick DK, Shaffer WO, Loeser JD (May 2009). "Surgery for low back pain: a review of the evidence for an American Pain Society Clinical Practice Guideline". Spine. 34 (10): 1094–109. Websites: www.spine-health.com www.webmd.com/back-pain/guide/back-pain-symptoms-types www.mayoclinic.org/diseases-conditions/back-pain/symptoms-causes/syc-20369906 Heart disease kills. Cardiovascular disease kills more men and more women each year than any other cause of death. Numbers of heart attacks and strokes, as well as episodes of congestive heart failure, are escalating to epidemic proportions. Prevention is the key to saving lives. Cardiovascular disease prevention focuses on risk factors. Risk factors are divided into two categories: Modifiable and Unmodifiable. Unmodifiable risk factors can't be changed. These include:
Gender. Men develop heart disease earlier than women. It is commonly thought that women lag behind in the development of heart disease by about ten years. However, more women are developing heart disease at an earlier age that ever before and often have more severe disease and symptoms that are very atypical. Family history of heart disease is a key predictor. This includes a close (parents or siblings) male relative having heart disease or a heart attack before the age of 55, and/or a female relative before the age of 65. Modifiable risk factors depend on you. These are things that you can change. If you have unmodifiable risk factors, it is very important that you minimize your risk of cardiovascular disease by modifying the factors listed below.
High blood pressure, or hypertension, causes the heart to work harder. Like any pump- the heart has to overcome the pressure against it. Because of this, the heart muscle can enlarge. High blood pressure can also damage the lining of the artery walls, which encourages plaque build-up. High blood pressure is defined by a blood pressure reading of 130/80 or greater. A healthy blood pressure is 120/80 or less. If you have other risk factors, even a blood pressure of 130/80 may be too high. High cholesterol. There are two types of cholesterol in the body: LDL and HDL. LDL - or "bad" - cholesterol sticks to the inside of an artery's walls, causing plaque to build up. HDL - or "good" - cholesterol circulates through the arteries and decreases the risk of plaque build-up. Cholesterol is found only in foods derived from animals, such as milk, cheese and meat. If you have an HDL cholesterol level of 60 or higher, your risk of heart disease does not increase, and may even be below average. This is true even if your total cholesterol levels are also high (greater than 200.) It's important to have both your total cholesterol and your cholesterol profile checked and evaluated in terms of your personal cardiovascular risk. The general goals for cholesterol levels are as follows: 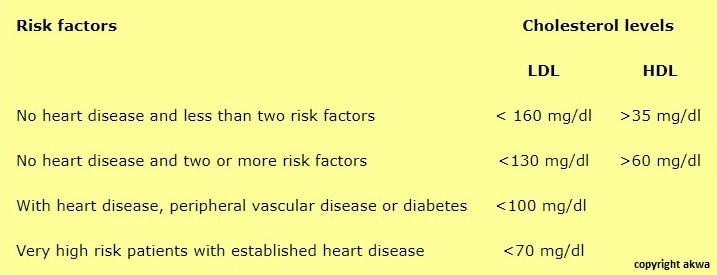 cholesterol levels Diabetes: Diabetes increases the rate at which heart disease develops and progresses. It is very important to get screened for diabetes. If you have diabetes, it is important to control your blood sugars well, exercise, and avoid any other risk factors. People with diabetes are at very high risk for cardiovascular disease and are often treated as if they have cardiovascular disease. If you have diabetes, it is imperative that you follow regularly with your doctor and report any symptoms that you may be having, such as chest pain or shortness of breath.
Stress puts excess demand on the heart muscle. During stressful situations, the body releases adrenaline, a hormone that increases heart rate and narrows blood vessels. This in turn increases blood pressure, and the heart works even harder. Stress does not need to be eliminated from life, but it can be reduced and controlled through stress management techniques and exercise. Obesity is one of the fastest growing health problems in the United States - for children and for adults. Regular physical activity and following a heart-healthy diet are a key prescription in the prevention and treatment of obesity and heart disease. Warding off heart disease on your own.Keeping your blood sugar levels under control, increasing your level of "good" cholesterol with regular exercise, maintaining a normal weight and, if you have it, controlling your high blood pressure are all good ways to help prevent heart disease. Also, aerobic exercise most if not all days of the week can help you to control the modifiable risk factors for heart disease. Before beginning any new exercise program, consult your physician and get screened for any risk factors for heart disease. By being aware of any risk factors, you and your physician can be proactive in your health care and reduce risks for heart disease. Be aware - it's your heart! Take the American Heart Association's quiz to see if you are at risk for a heart attack. Christiaan Janssens CRO Akwa Wellness Sources and References: Swerdlow, Daniel I.; Humphries, Steve E. (2017-02-01). "Genetics of CHD in 2016: Common and rare genetic variants and risk of CHD". Nature Reviews Cardiology. 14 (2): 73–74. Ronksley, Paul E.; Brien, Susan E.; Turner, Barbara J.; Mukamal, Kenneth J.; Ghali, William A. (2011-02-22). "Association of alcohol consumption with selected cardiovascular disease outcomes: a systematic review and meta-analysis". BMJ. 342: d671. Ignarro, LJ; Balestrieri, ML; Napoli, C (Jan 15, 2007). "Nutrition, physical activity, and cardiovascular disease: an update". Cardiovascular Research. 73 (2): 326–40. Bhupathiraju, SN; Tucker, KL (Aug 17, 2011). "Coronary heart disease prevention: nutrients, foods, and dietary patterns". Clinica Chimica Acta. 412 (17–18): 1493–514. Vanhecke TE, Miller WM, Franklin BA, Weber JE, McCullough PA (Oct 2006). "Awareness, knowledge, and perception of heart disease among adolescents". Eur J Cardiovasc Prev Rehabil. 13 (5): 718–23. World Health Organization (2008). Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health : Commission on Social Determinants of Health Final Report. World Health Organization. Berneis K, Rizzo M. "LDL size: does it matter?" Swiss Med Wkly 2004;134:720-724. Websites: https://www.hart-en-vaatziekten.com/ https://www.rug.nl/about-us/news-and-events/events/phd-ceremonies/?hfId=2500  Hypertension? Hypertension? Blood pressure is the pressure created by the heart as it pumps blood through the arteries and the circulatory system. What blood pressure numbers mean
What High Blood Pressure Does to the Body High blood pressure puts you at a higher risk for the following:
Symptoms of High Blood Pressure High blood pressure usually has NO SYMPTOMS!! Because of this it is sometimes referred to as "The Silent Killer". How to tell if you might have high blood pressure:
Causes of High Blood Pressure Blood pressure develops when certain nerve impulses cause arteries to become larger (dilate) or smaller (contract). If vessels are wide open blood flows easily. If vessels narrow pressure inside increases causing hypertension. The cause of vessels narrowing is unknown in 90 to 95% of cases. This is called Primary Hypertension. In 5 to 10% of cases, the cause of vessel narrowing comes from another condition. This is called Secondary Hypertension. Some common conditions that can cause secondary hypertension are:
Risk Factors of High Blood Pressure Risk Factors You Can't Control Uncontrollable risk factors are inherent to you and cannot be changed. They include:
Controllable risk factors are lifestyle choices that increase the risk of high blood pressure. They include:
Women and High Bood Pressure Women are particularly at risk for hypertension due to the following:
What You Can Do to Reduce the Risk of Hypertension High blood pressure is a lifelong disease. It can be controlled, but not cured. Controlling blood pressure will reduce the risk of stroke, heart attack, heart failure and kidney disease. The following lifestyle changes will help you reduce your risk:
The Ten Commandments for Blood Pressure Control
Medication for High Blood Pressure
Blood Pressure Measurement Blood pressure is measured using a sphygmomanometer. There are two numbers in a bood pressure reading.
American Heart Association Recommended Blood Pressure Levels   Copyright Akwa Wellness Home Blood Pressure Monitoring Mercury sphygmomanometer
Drs. Christiaan Janssens MBA CRO Akwa Wellness Sources and References:
Rowan, Robert; Schrader, Constance, Control High Blood Pressure Without Drugs: A Complete Hypertension Handbook (2001). James, Paul A.; Oparil, Suzanne; Carter, Barry L.; Cushman, William C.; Dennison-Himmelfarb, Cheryl; Handler, Joel; Lackland, Daniel T.; Lefevre, Michael L.; MacKenzie, Thomas D.; Ogedegbe, Olugbenga; Smith, Sidney C.; Svetkey, Laura P.; Taler, Sandra J.; Townsend, Raymond R.; Wright, Jackson T.; Narva, Andrew S.; Ortiz, Eduardo (18 December 2013). "2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults". JAMA. 311 (5): 507–20. Lackland, DT; Weber, MA (May 2015). "Global burden of cardiovascular disease and stroke: hypertension at the core". The Canadian journal of cardiology. 31 (5): 569–71. Mendis, Shanthi; Puska, Pekka; Norrving, Bo (2011). Global atlas on cardiovascular disease prevention and control (PDF) (1st ed.). Geneva: World Health Organization in collaboration with the World Heart Federation and the World Stroke Organization. p. 38. ISBN 9789241564373. Hernandorena, I; Duron, E; Vidal, JS; Hanon, O (July 2017). "Treatment options and considerations for hypertensive patients to prevent dementia". Expert Opinion on Pharmacotherapy (Review). 18 (10): 989–1000. Poulter, NR; Prabhakaran, D; Caulfield, M (22 August 2015). "Hypertension". Lancet. 386 (9995): 801–12. doi:10.1016/s0140-6736(14)61468-9. Carretero OA, Oparil S; Oparil (January 2000). "Essential hypertension. Part I: definition and etiology". Circulation. 101 (3): 329–35. doi:10.1161/01.CIR.101.3.329. "How Is High Blood Pressure Treated?". National Heart, Lung, and Blood Institute. 10 September 2015. Campbell, NR; Lackland, DT; Lisheng, L; Niebylski, ML; Nilsson, PM; Zhang, XH (March 2015). "Using the Global Burden of Disease study to assist development of nation-specific fact sheets to promote prevention and control of hypertension and reduction in dietary salt: a resource from the World Hypertension League". Journal of clinical hypertension (Greenwich, Conn.). 17 (3): 165–67. Naish, Jeannette; Court, Denise Syndercombe (2014). Medical sciences (2 ed.). p. 562. ISBN 9780702052491. Lau, DH; Nattel, S; Kalman, JM; Sanders, P (August 2017). "Modifiable Risk Factors and Atrial Fibrillation". Circulation (Review). 136 (6): 583–96. James, PA.; Oparil, S.; Carter, BL.; Cushman, WC.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, DT.; Lefevre, ML.; et al. (Dec 2013). "2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8)". JAMA. 311 (5): 507–20. Musini, VM; Tejani, AM; Bassett, K; Wright, JM (7 October 2009). "Pharmacotherapy for hypertension in the elderly". The Cochrane Database of Systematic Reviews (4): CD000028. Sundström, Johan; Arima, Hisatomi; Jackson, Rod; Turnbull, Fiona; Rahimi, Kazem; Chalmers, John; Woodward, Mark; Neal, Bruce (February 2015). "Effects of Blood Pressure Reduction in Mild Hypertension". Annals of Internal Medicine. 162: 184–91. Xie, X; Atkins, E; Lv, J; Bennett, A; Neal, B; Ninomiya, T; Woodward, M; MacMahon, S; Turnbull, F; Hillis, GS; Chalmers, J; Mant, J; Salam, A; Rahimi, K; Perkovic, V; Rodgers, A (30 January 2016). "Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: updated systematic review and meta-analysis". Lancet. 387 (10017): 435–43 Diao, D; Wright, JM; Cundiff, DK; Gueyffier, F (Aug 15, 2012). "Pharmacotherapy for mild hypertension". The Cochrane Database of Systematic Reviews. 8: CD006742. Garrison, SR; Kolber, MR; Korownyk, CS; McCracken, RK; Heran, BS; Allan, GM (8 August 2017). "Blood pressure targets for hypertension in older adults". The Cochrane Database of Systematic Reviews. Websites: http://newsroom.cumc.columbia.edu/blog/2018/02/14/understanding-the-new-blood-pressure-treatment-guidelines/ https://www.medicalnewstoday.com/articles/159283.php https://www.health.harvard.edu/topics/blood-pressure https://www.healthyhorns.utexas.edu/HT/HT_highbloodpressure.html http://www.acc.org/latest-in-cardiology/articles/2017/11/08/11/47/mon-5pm-bp-guideline-aha-2017 |
AuthorDrs. Christiaan Janssens Archive
Augustus 2019
Categories |
 RSS-feed
RSS-feed
